|
Tenosinovitis
Definition
This term describes the inflammation of the synovial sheath that surrounds the tendon (fig 1). In climbing, it refers to the inflammation of a synovial sheath that surrounds the tendons of the flexors of the fingers.
It usually appears suddenly, with acute pain around the first phalanx (P1). It is possible to have the pain radiate to the palm or even to the forearm. Sometimes you can see an oedema at P1 level.
It is often mixed up wrongly with a pulley rupture because of its sudden appearance but it is not as serious as a pulley rupture. However, it should not be left untreated.
A comparison can be made between the state of the sheath during a tenosynovitis and the state of the skin during a “steak”: imagine the little bleeding of the sheath and you will understand why it hurts
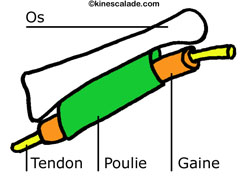
Fig 1: Situation of the sheath
Mechanism of the lesion
It appears during a crushing of the sheath between the pulley and the tendon or between the hold and the tendon.
It is the result of an intense mechanical impact that occurs only once or less intense impact that occurs repeatedly.
It is important to take into account that the repetition of the movement is really harmful for the structures.
When holding a crimp, the sheath is crushed between the tendon and the pulley (fig 2).
When grabbing an angular hold with an open hand grip, the sheath is pinched between the rock and the tendon, such as the bone (fig 3).
 |
Fig 2: Friction between the pulley and the tendon |
 |
Fig 3: Friction between the tendon and an angular hold |
Prevention
Technique correction:
Use open hand holds and slopers with an open hand grip, avoid angular holds or hold them in a way that is non-traumatizing.
Correction of the exercise schedule:
Respect the fact that progress is gradual, do not train too hard without rest, adjust the intensity and the work-out to your level.
You need to spend a period of 3 weeks with maximum the strength and the resistance training.
Correction of the physical preparation:
Progressive training of the muscles of the fingers before starting a maximum project, especially for one-finger, two-finger holds or crimps.
Warm-up and stretching exercises you should never forget.
Treatment
Stop the session.
Put ice on it the fastest you can. Then apply an anti-inflammatory gel.
Do not use you finger as long as the pain persists at rest.
Put on a ring of strappal® (fig 4), which enables you only to take open hand holds and keep it on day and night for ten days. Change it every day; put ice on it and then again the anti-inflammatory gel.

Fig 4: Tapping of the finger
Take up training again but do not use traumatic holds (open hand grip on angular and crimp holds) and avoid all pain (if it hurts: stop).
See the sport doctor if the symptoms persist (no infiltration).
Some physical therapy sessions with ultrasound can accelerate the healing.
|